Americans Pay Almost Double for Health Care
The United States has the most expensive health-care system in the world, but when comparing our population health with our international peers we have poor health outcomes.

Despite its high spending on health care, the U.S. has poor population health.
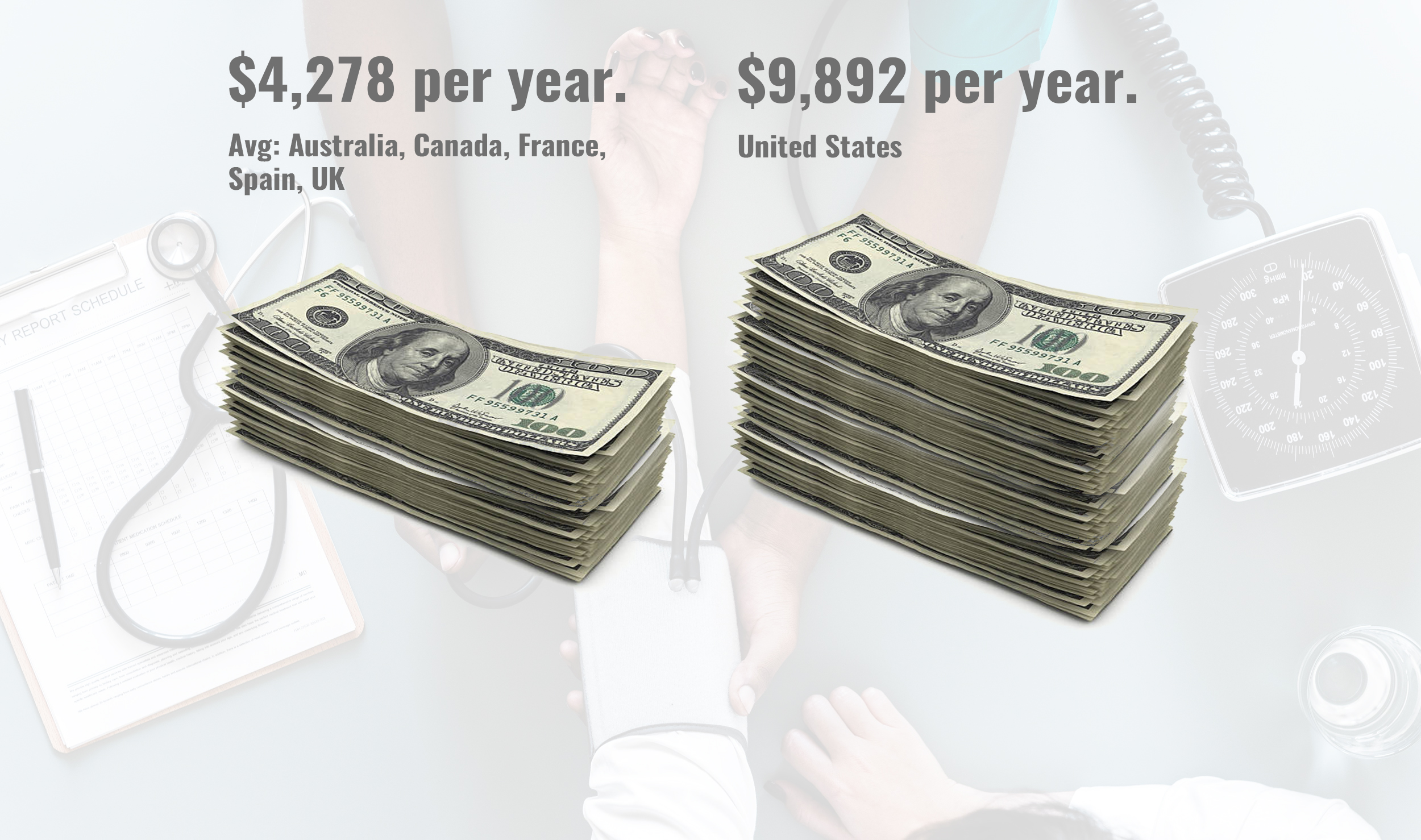
 On average, other wealthy countries spend about half as much per person on health expenditures than the U.S. spends. According to the Organization for Economic Cooperation and Development (OECD) in 2016 the total health expenditures per capita in the U.S. was $10,348, twice that of the median health expenditures of $5,169 for other wealthy countries. Keep in mind that the other advanced nations provide comprehensive coverage to their entire populations, while the U.S. leaves 51 million completely uninsured and millions more with inadequate coverage.
On average, other wealthy countries spend about half as much per person on health expenditures than the U.S. spends. According to the Organization for Economic Cooperation and Development (OECD) in 2016 the total health expenditures per capita in the U.S. was $10,348, twice that of the median health expenditures of $5,169 for other wealthy countries. Keep in mind that the other advanced nations provide comprehensive coverage to their entire populations, while the U.S. leaves 51 million completely uninsured and millions more with inadequate coverage.
Despite paying twice as much for health expenditures the U.S. has a lower life expectancy than other developed nations. The average life expectancy for Americans is 78.7 years, which puts the US 1.5 years lower than the OECD median life expectancy of 80.3 years.
Another widely-utilized indicator of population health, the infant mortality rate (death within their first year of life), is extremely high in the U.S. Our infant mortality rate is 5.8 deaths per 1,000 live births in 2014, while the rate among comparable countries, was 3.4 deaths. Overall, the U.S. and comparable countries have seen a decrease in infant mortality rate in recent years, but the rate is decreasing in other countries at a much higher pace, almost double.
Americans spend more on health care and get less
One reason we spend more and get less than the rest of the world is because we have a patchwork system of for-profit payers. Private insurers spend health dollars on things that have nothing to do with care: overhead, underwriting, billing, sales and marketing departments as well as huge profits and exorbitant executive pay. Blue Cross Blue Shield of Michigan’s top executive received a compensation of $13.4 million in 2017. That’s just one CEO, at one insurance company, in one state.
This massive system of multiple for-profit entities means that doctors and hospitals must maintain costly administrative staffs to deal with the bureaucracy. As a result, administration alone consumes at least 25 percent of Americans’ health dollars, most of which is waste.
David Cutler, a health economist in the United States, provided an example of a heavy administration when he revealed that, “Duke University Hospital has 900 hospital beds and 1,300 billing clerks. The typical Canadian hospital has a handful of billing clerks. Single-payer systems have fewer administrative needs.”
Americans pay more for health-care services
Another reason Americans pay more and get less is because we literally pay more for the technology (such as MRIs, CTs, etc.), pharmaceuticals and procedures.
A 2016 report by Kaiser Family Foundation (an analysis of data from International Federation of Health Plans, 2015) offers evidence of the high prices paid by Americans compared to other developed countries.
- For instance, the average cost of an MRI in the U.S. was $1,119 in 2015. An MRI in Spain averaged $130.
- The average cost of an appendectomy: $15,930 in the U.S, $8,009 in the United Kingdom, and $3,814 in Australia.
- The average cost of a normal delivery of a baby: $10,808 in the U.S. compared to $7,751 in Switzerland and $5,312 in Australia.
- Bills for hip replacement averaged $29,067 in the U.S. compared to $19,484 in the U.K. and $6,757 in Spain, the study said.
Americans pay more for pharmaceuticals
The same report offers examples of prescription drugs that also cost more in the U.S.
- A month’s supply of Humira, a drug to treat rheumatoid arthritis averaged $2,669 in the U.S. compared to $1,362 in the U.K. and $822 in Switzerland.
- A month’s supply of Avastin, a cancer drug, averaged $3,930 in the U.S. compared to $1,752 in Switzerland and $480 in the U.K.
- A month’s supply of Xarelto, a drug to treat blood clots averaged $292 in the U.S. compared to $126 in the U.K. and $48 in South Africa.
- A Single-payer national system is the only way to avoid wasting $400 billion in administration costs, while bringing down the cost of pharmaceuticals and controlling the costs of care. The savings obtained from replacing today’s inefficient, profit-oriented, multiple insurance payers with a single streamlined, nonprofit, public payer would fund the single payer program along with some modest new taxes based on ability to pay. Premiums would disappear, and it’s predicted that 95 percent of all households would save money.
What is Single Payer?
According to Physicians for a National Health System (PNHP), “Single-payer national health insurance, also known as ‘Medicare for all,’ is a system in which a single public or quasi-public agency organizes health care financing, but the delivery of care remains largely in private hands. Under a single-payer system, all residents of the U.S. would be covered for all medically necessary services, including doctor, hospital, preventive, long-term care, mental health, reproductive health care, dental, vision, prescription drug and medical supply costs.”
Patients would no longer face financial barriers to care such as co-pays and deductibles and would regain free choice of doctor and hospital. Doctors would regain autonomy over patient care.
Physicians would be paid on a fee-for-service basis according to a negotiated formulary or receive a salary from a hospital or nonprofit HMO/group practice. Hospitals would receive a global budget for operating expenses. Health facilities and expensive equipment purchases would be managed by regional health planning boards.
A single-payer system would be financed by eliminating private insurers and recapturing their administrative waste. Modest new taxes, based on ability to pay, would replace premiums and out-of-pocket payments currently paid by individuals and business. Costs would be controlled through negotiated fees, global budgeting and bulk purchasing.
Can you imagine how much money Americans would save with a single payer system just by deleting the need for exorbitant executive pay, negotiating nationally for bulk pharmaceutical purchase prices like other countries do, standardizing fees, and cutting the need for the multi-payer administration fees? And every American would have health care.

Medical Care and the Health Risks Forced Upon Women by Abortion Bans
Between a Rock and a Hard Place Much of the political debate about abortion in America focuses on abortions performed late in pregnancy, but the overwhelming majority of them occur in the first trimester. Forty-three percent of all abortions occur in the first six...

Myth: Universal Healthcare in America Would be Very Expensive
Myth: Universal Healthcare in America Would be Very Expensive Healthcare is like education: everybody needs it, regardless of their budget, but it’s expensive. That’s why all advanced economies, except the United States, fund it through taxation. Julianna Truesdale...

The more steps you and your family can take to prevent the spread of COVID-19, the safer you and your loved ones will be.
Mask Up! Many People With COVID-19 Do Not Know They Have It!Your Loved One Could Become Seriously Sick or Die from COVID-19Julianna TruesdaleWhy is it important to wear a mask around my relatives? COVID-19 cases and deaths are rising across...

Do you know why United States Healthcare costs are so high?
Do you know why United States Healthcare costs are so high? Julianna Truesdale Americans have reached a new high in support for having presidential elections based on the popular vote instead of the Electoral College. While most Americans –...